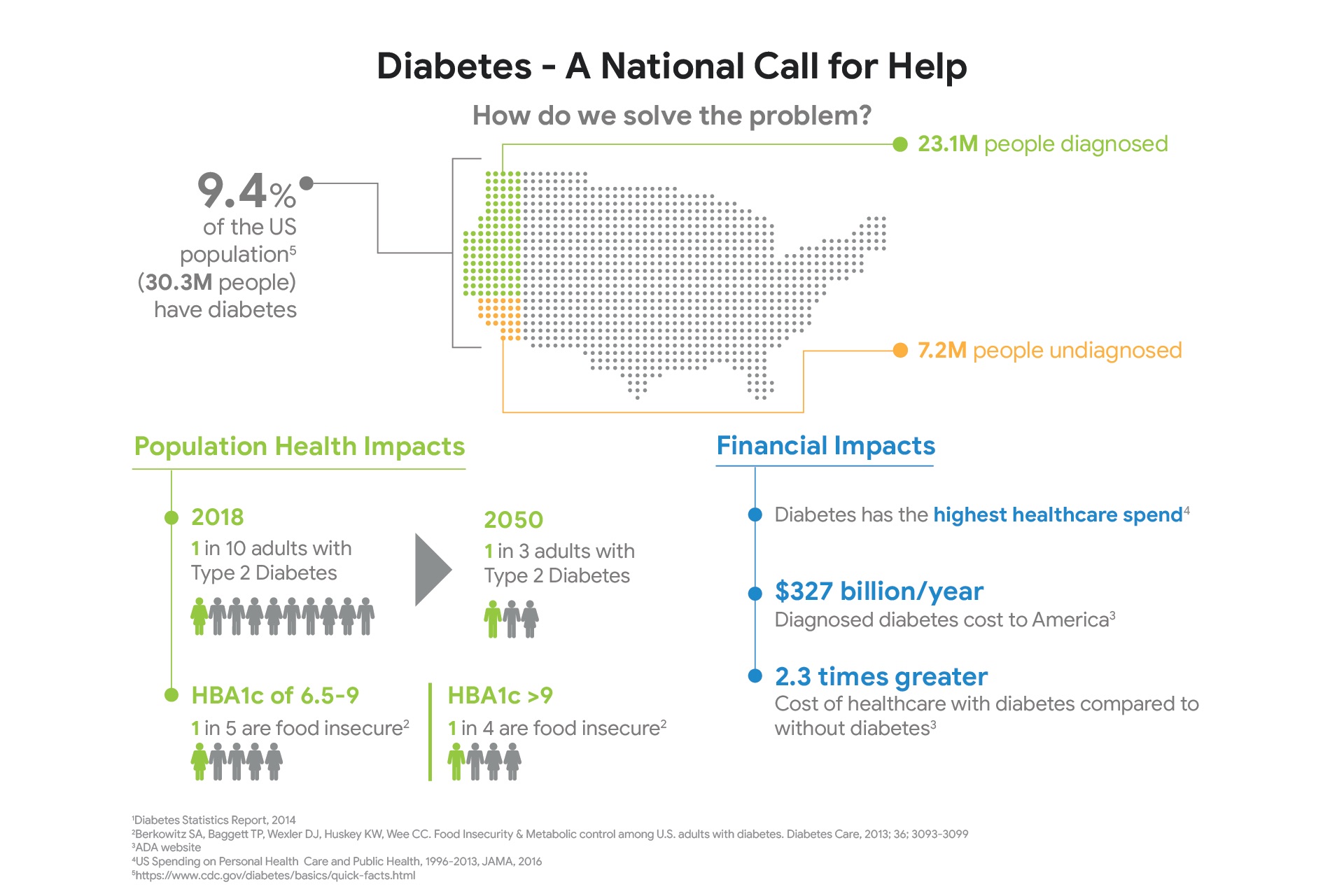
And Americans are sick — much sicker than many realize. More than 100 million adults — almost half the entire adult population — have pre-diabetes or diabetes. Cardiovascular disease afflicts about 122 million people and causes roughly 840,000 deaths each year, or about 2,300 deaths each day. Three in four adults are overweight or obese. More Americans are sick, in other words, than are healthy.
Instead of debating who should pay for all this, no one is asking the far more simple and imperative question: What is making us so sick, and how can we reverse this so we need less health care? The answer is staring us in the face, on average three times a day: our food.
Poor diet is the leading cause of mortality in the United States, causing more than half a million deaths per year. Just 10 dietary factors are estimated to cause nearly 1,000 deaths every day from heart disease, stroke and diabetes alone. These conditions are dizzyingly expensive. Cardiovascular disease costs $351 billion annually in health care spending and lost productivity, while diabetes costs $327 billion annually. The total economic cost of obesity is estimated at $1.72 trillion per year, or 9.3 percent of gross domestic product.
These human and economic costs are leading drivers of ever-rising health care spending, strangled government budgets, diminished competitiveness of American business and reduced military readiness.
Fortunately, advances in nutrition science and policy now provide a road map for addressing this national nutrition crisis. The “Food Is Medicine” solutions are win-win, promoting better well-being, lower health care costs, greater sustainability, reduced disparities among population groups, improved economic competitiveness and greater national security.
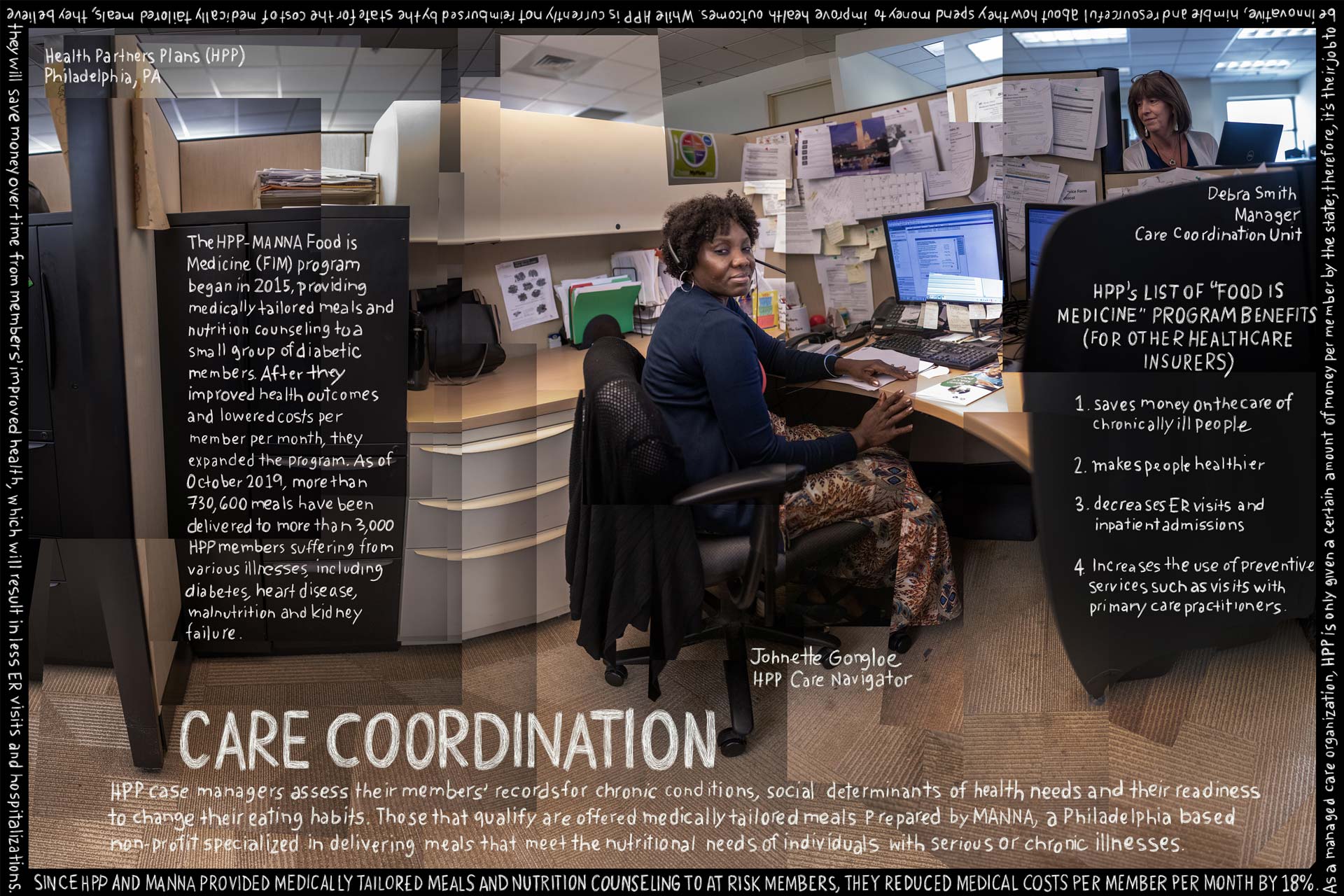
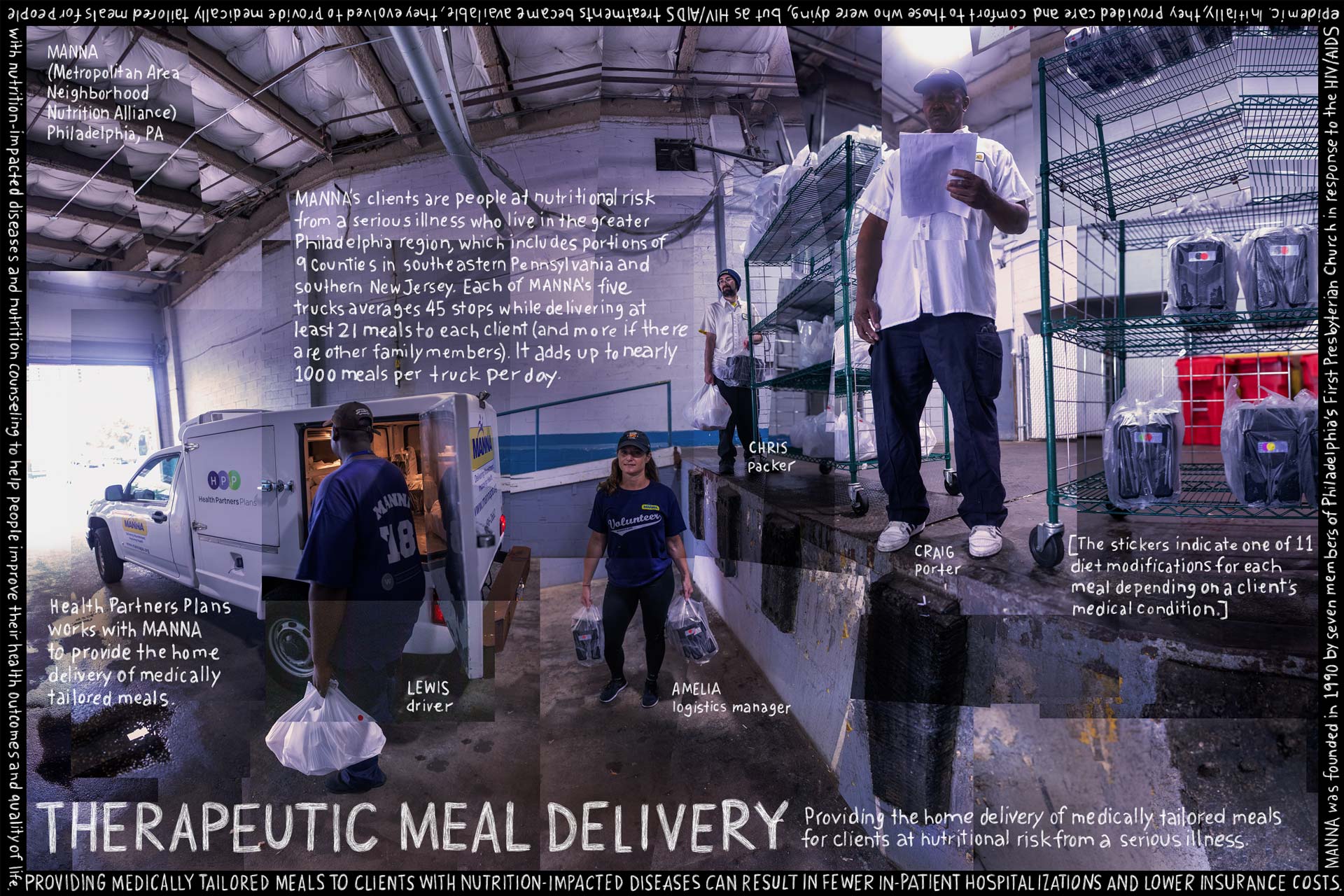
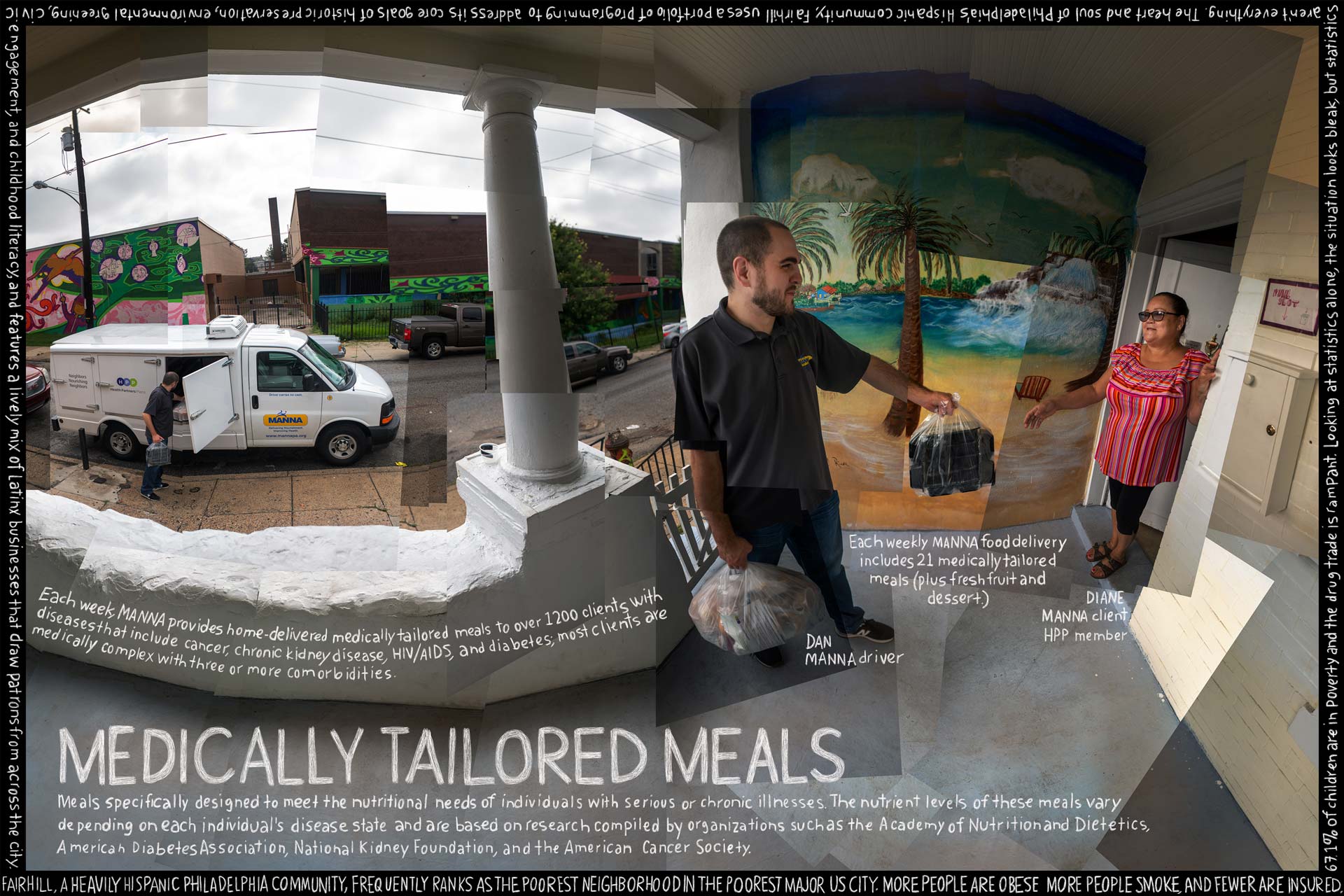
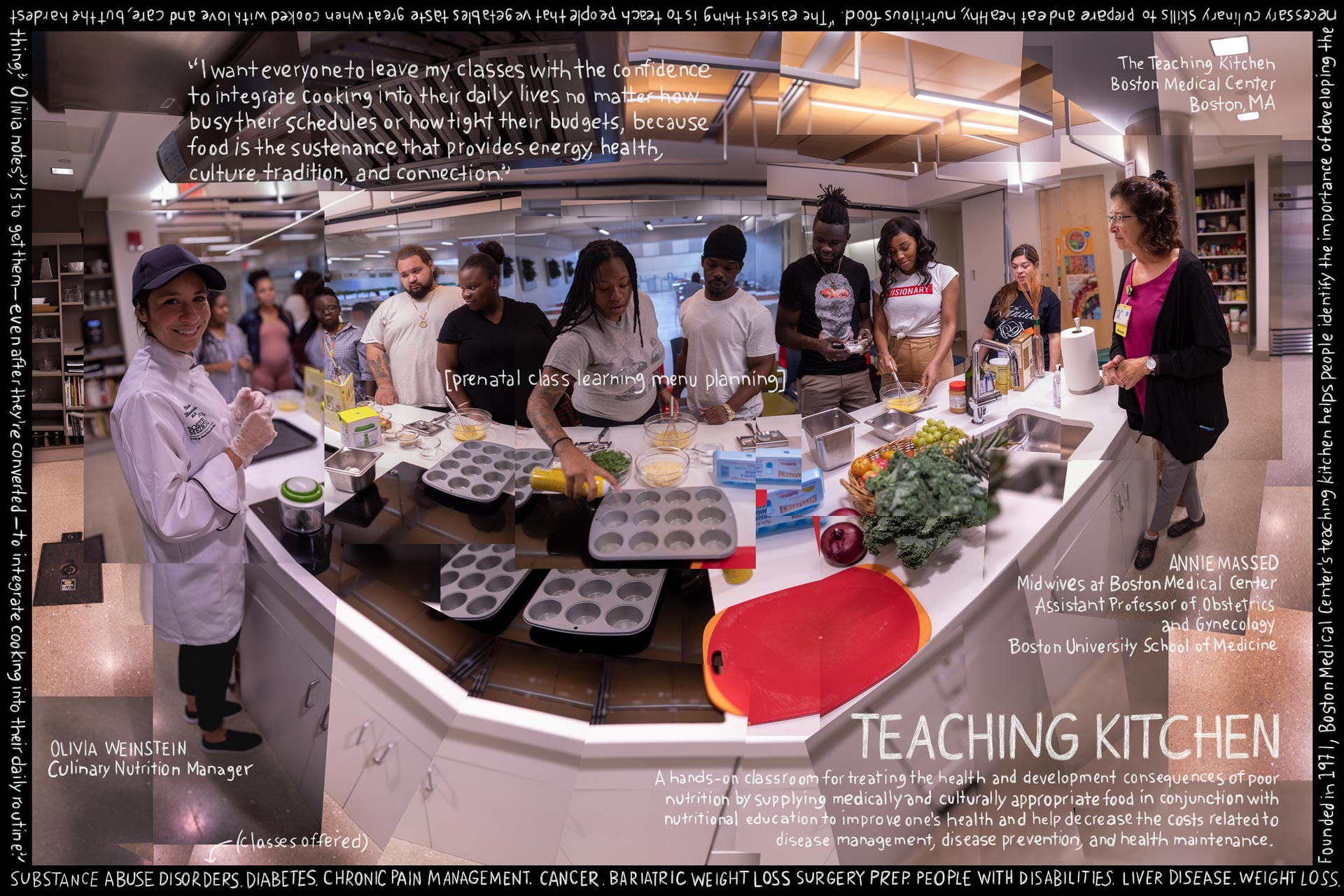
Some simple, measurable improvements can be made in several health and related areas. For example, Medicare, Medicaid, private insurers and hospitals should include nutrition in any electronic health record; update medical training, licensing and continuing education guidelines to put an emphasis on nutrition; offer patient prescription programs for healthy produce; and, for the sickest patients, cover home-delivered, medically tailored meals. Just the last action, for example, can save a net $9,000 in health care costs per patient per year.
Nutrition standards in schools, which have improved the quality of school meals by 41 percent, should be strengthened; the national Fresh Fruit and Vegetable Program should be extended beyond elementary schools to middle and high schools; and school garden programs should be expanded. And the Supplemental Nutrition Assistance Program, which supports grocery purchases for nearly one in eight Americans, should be leveraged to help improve diet quality and health.
Coordinated federal leadership and funding for research is also essential. This could include, for example, a new National Institute of Nutrition at the National Institutes of Health. Without such an effort, it could take many decades to understand and utilize exciting new areas, including related to food processing, the gut microbiome, allergies and autoimmune disorders, cancer, brain health, treatment of battlefield injuries and effects of nonnutritive sweeteners and personalized nutrition.
Finally, Government plays a crucial role. The significant impacts of the food system on well-being, health care spending, the economy and the environment — together with mounting public and industry awareness of these issues — have created an opportunity for government leaders to champion real solutions.






















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}